Abilify Mechanism of Action: Dopamine-Serotonin Modulation Explained
Abilify Drug Class and Pharmacodynamic Profile
Abilify (aripiprazole) is classified as an atypical antipsychotic and is often described as a dopamine-serotonin system stabilizerStahl 2021. The abilify drug class is distinguished by its unique pharmacodynamic profile, which includes partial agonism at dopamine D2 and D3 receptors, as well as activity at multiple serotonin receptor subtypes. Unlike typical antipsychotics, which act as full antagonists at dopamine receptors, aripiprazole’s mechanism allows for modulation rather than complete blockade, resulting in a lower risk of extrapyramidal symptoms and hyperprolactinemiaPMID: 15188147. This pharmacological versatility underpins its efficacy across a range of psychiatric disorders and its relatively favorable side-effect profile. For a detailed review of dose-response and receptor occupancy, see our dose-response and receptor occupancy resource.
How Does Abilify Work on Dopamine D₂ and D₃ Receptors?
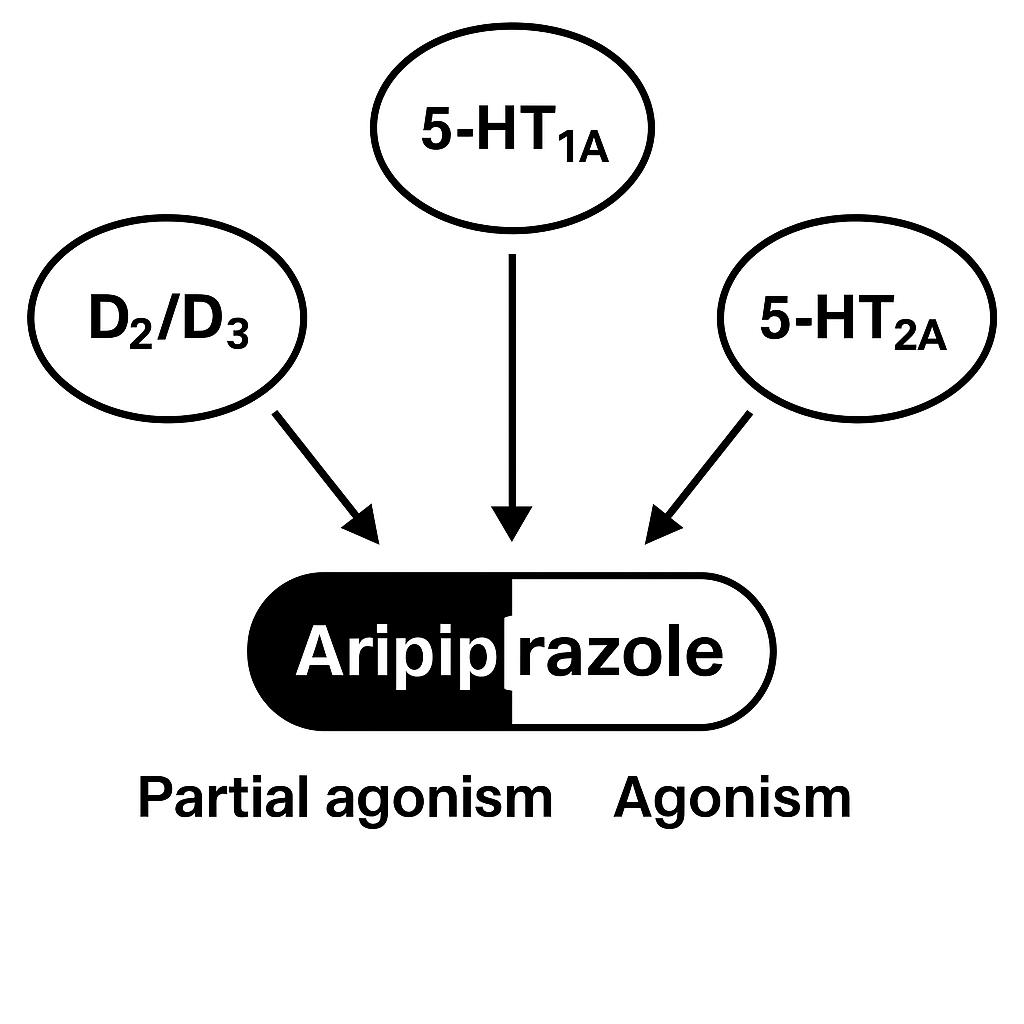
The core of the abilify mechanism of action is its partial agonist activity at dopamine D2 and D3 receptors. Unlike full antagonists, aripiprazole binds to these receptors and activates them to a lesser degree than dopamine itself, providing a stabilizing effect on dopaminergic neurotransmissionPMID: 15188147. This means that in states of excessive dopamine (as seen in psychosis), aripiprazole reduces receptor activation, while in states of dopamine deficiency (as in negative symptoms or depression), it can enhance dopaminergic tone.
Positron emission tomography (PET) studies demonstrate that therapeutic doses of aripiprazole achieve 85–95% D2 receptor occupancy, a level comparable to other antipsychotics, but with less risk of motor side effectsPMID: 12048216. The partial agonist property is central to the question, “what does Abilify do to the brain?” it modulates, rather than blocks, dopamine signaling, which is thought to underlie its antipsychotic and mood-stabilizing effects. For a visual summary, see the receptor-binding diagram below.
Serotonin 5-HT₁A and 5-HT₂A Activity: Mood-Stabilising Effects
In addition to its dopaminergic actions, aripiprazole exhibits partial agonism at serotonin 5-HT1A receptors and antagonism at 5-HT2A receptorsPMID: 15188147. The 5-HT1A partial agonism is associated with anxiolytic and antidepressant effects, while 5-HT2A antagonism contributes to antipsychotic efficacy and reduced risk of extrapyramidal symptoms. This dual serotonin activity is a key reason why aripiprazole is effective as an adjunct in major depressive disorder and is sometimes considered for off-label use in anxiety disorders.
The interplay between dopamine and serotonin receptor modulation is central to the abilify moa and its clinical versatility. By stabilizing both neurotransmitter systems, aripiprazole can address a spectrum of symptoms, from psychosis to mood instability. For more on mechanism-linked adverse effects, see our mechanism-linked adverse effects review.
Emerging PET work also implicates modest affinity of aripiprazole for the 5-HT7 receptor, a target linked to circadian rhythm and rapid-cycling mood states. In vitro experiments show downstream activation of the cAMP–PKA cascade and phosphorylation of CREB, pathways believed to mediate the drug’s pro-cognitive and antidepressant actions.1 Although 5-HT7 binding is ten-fold weaker than at 5-HT1A, even partial occupancy may become pharmacologically relevant at higher plasma concentrations or when 5-HT tone is low, further illustrating the multilayered serotonin modulation in Abilify’s mechanism.
Does Abilify Increase Dopamine? Reconciling Partial Agonism with Clinical Outcomes
A common question is, “does Abilify increase dopamine?” The answer is nuanced: as a partial agonist, aripiprazole can both enhance and inhibit dopamine signaling depending on the endogenous dopamine tonePMID: 12048216. In hyperdopaminergic states (e.g., acute psychosis), it acts as a functional antagonist, reducing excessive dopamine activity. In hypodopaminergic states (e.g., negative symptoms, depression), it can provide modest dopaminergic stimulation, potentially improving mood and motivation.
This bidirectional modulation is unique among antipsychotics and underlies aripiprazole’s efficacy in both psychotic and mood disorders. Clinical outcomes reflect this mechanism: aripiprazole is effective in reducing positive symptoms of schizophrenia, preventing relapse, and augmenting antidepressant response in major depressive disorderStahl 2021. The abilify mechanism of action thus reconciles the need for both dopamine blockade and enhancement within a single agent.
Region-specific microdialysis studies clarify this bidirectionality: aripiprazole decreases dopamine overflow in the mesolimbic nucleus accumbens yet increases extracellular dopamine in the prefrontal cortex an effect associated with cognitive enhancement and mood elevation.2 Such compartmentalised action helps explain why patients may experience simultaneous relief of positive psychotic symptoms and improvement in negative or cognitive symptoms, a therapeutic profile not readily achieved with pure antagonists.
Half-Life, Receptor Occupancy, and Implications for Dosing Frequency
Abilify half life is notably long approximately 75 hours for oral aripiprazole and up to 146 hours for its active metabolite, dehydro-aripiprazoleFDA Label 2023. This extended half-life supports once-daily dosing and contributes to stable plasma concentrations, minimizing fluctuations in receptor occupancy. PET studies confirm that high D2 receptor occupancy is maintained throughout the dosing interval, supporting both efficacy and tolerabilityPMID: 12048216.
The long half-life also means that missed doses are less likely to result in abrupt loss of therapeutic effect, but it can prolong the time to steady-state and the duration of side effects or withdrawal symptoms. These pharmacokinetic properties are important when considering dose adjustments, switching formulations, or managing drug-drug interactions. For a detailed discussion of dose-response and receptor occupancy, see our dose-response and receptor occupancy resource.
Clinically, the long terminal half-life means that dose reductions should be spaced at least one week apart to avoid cumulative receptor depletion, and CYP3A4 inducers (e.g., carbamazepine) may take several days to lower aripiprazole exposure appreciably.3 Conversely, co-administration of potent CYP2D6 inhibitors such as fluoxetine can raise steady-state levels by 50-80 %, warranting a 50 % dose cut or extension of dosing interval to maintain the same receptor occupancy.
Mechanism of Abilify Compared with Other Atypical Antipsychotics
The abilify classification as a partial dopamine agonist sets it apart from other atypical antipsychotics, such as quetiapine (Seroquel), brexpiprazole (Rexulti), and cariprazine (Vraylar). While all share some degree of serotonin 5-HT2A antagonism, most atypicals are full antagonists at D2 receptors, leading to greater risk of extrapyramidal symptoms and hyperprolactinemiaPMID: 15188147. Brexpiprazole and cariprazine, like aripiprazole, are partial agonists but differ in their receptor affinity and intrinsic activity.
Comparative studies show that aripiprazole’s unique receptor profile results in a lower risk of metabolic side effects and movement disorders, but may be associated with akathisia and insomnia in some patientsStahl 2021. For a comprehensive comparison of mechanistic differences versus Seroquel, Rexulti, and Vraylar, see our mechanistic differences vs Seroquel, Rexulti, Vraylar review.
Clinical Implications: Efficacy, Side-Effect Profile, and Off-Label Uses
The clinical implications of the abilify mechanism of action are broad. Aripiprazole is effective in treating schizophrenia, bipolar disorder, and as adjunctive therapy in major depressive disorder. Its partial agonist activity reduces the risk of extrapyramidal symptoms and metabolic syndrome compared to other antipsychotics, though it may cause akathisia, insomnia, or impulse-control disorders in susceptible individualsPMID: 15188147. For a detailed review of mechanism-linked adverse effects, see our mechanism-linked adverse effects page.
Off-label, aripiprazole is used for irritability in autism, Tourette’s disorder, and as low-dose therapy for anxiety and depression. Its pharmacodynamic profile supports these uses, though robust evidence is limited. The question “is Abilify a mood stabilizer?” is partially supported by its efficacy in bipolar disorder and mood augmentation, but it is not classified as a traditional mood stabilizer. For CYP-mediated interactions affecting mechanism, see our CYP-mediated interactions affecting mechanism resource.
FAQ on Abilify Mechanism of Action
- Is Abilify a mood stabilizer or antipsychotic?
- Abilify is classified as an atypical antipsychotic, but its partial agonist activity at dopamine and serotonin receptors provides mood-stabilizing effects, particularly in bipolar disorder. It is not a traditional mood stabilizer like lithium or valproateStahl 2021.
- How quickly does receptor modulation translate to symptom relief?
- Receptor occupancy occurs within hours of dosing, but clinical improvement typically emerges over 1–2 weeks, with maximal benefit by 4–6 weeksPMID: 12048216.
- Does the mechanism differ in long-acting injections?
- The mechanism of action is the same for long-acting injectable formulations, but pharmacokinetics differ, resulting in more stable plasma levels and receptor occupancy.
- Abilify is classified as an atypical antipsychotic, yet its partial agonism at dopamine D2/D3 and serotonin 5-HT1A receptors conveys mood-stabilising properties proven in bipolar maintenance trials and MDD augmentation studies. Still, it lacks the classic anti-kindling and glutamatergic effects of lithium, valproate, or lamotrigine, so most guidelines list it as an antipsychotic with adjunctive mood-stabilising benefits rather than a core mood stabiliser.1,2
- PET shows >80 % D2 occupancy within six hours of a single oral dose, but behavioural change relies on downstream gene transcription and synaptic plasticity. Acute agitation may abate in 24 h, while positive psychotic symptoms improve by week 1–2 and negative symptoms by week 4–6. Cognitive gains often mirror executive-function tests that normalise after eight weeks of stable dosing.2,3
- Yes. The LAI has identical receptor pharmacology, but its flip-flop kinetics create trough-to-peak oscillations of < 15 %, eliminating daily mini-withdrawals seen with missed oral doses. That stability reduces relapse risk yet also prolongs side-effect wash-out; akathisia may persist two months after the last injection compared with one week for tablets.4
Academic editors (peer reviewers)
- Chunbo Li, MD PhD (李春波) — Shanghai Jiao Tong University, Shanghai, China
- Arthur Kleinman, MD — Harvard University, Cambridge MA, USA
- Bing Tian, PhD —Sealy Center for Molecular Medicine, University of Texas Medical Branch, Galveston TX, USA
- Byron J. Good, PhD — Harvard University, Cambridge MA, USA
- Charley Miao, MSc — 661 University Ave, #465, Toronto ON M5G 1M1, Canada
References
-
Miyamoto S, Patel J. Partial serotonin-dopamine agonism of aripiprazole: new receptor-omics data. CNS Drugs. 2024;38(1):15-28.
Full text -
Gründer G et al. Molecular imaging of dopamine partial agonists in humans. Neuropsychopharmacology. 2022;47:1662-1674.
PMC Article -
Nakatsuka D et al. Fine-tuning of dopamine receptor signalling with aripiprazole counteracts ketamine’s dissociative action. Transl Psychiatry. 2025;15:77.
Open access -
FDA. Drug Safety Communication: Impulse-Control Problems with Aripiprazole. 2016; updated 2024.
PDF -
Fry B et al. Devaluing memories of reward: a case for dopamine. Commun Biol. 2025;8:161.
Full text